joannakat said:
Really excellent article. Leaves very little to speculation. One thing it doesn't mention is whether symptoms are the same we're used to looking for. Since it's not mentioned, I'm going to assume they're the same. 
From a newsletter written by an epidemiologist that a former coworker and buddy follow. She is a home health therapist working exclusively with ventilated ALS patients who are being cared for at home. Very fragile patients…. so, she stays abreast and likes this particular source for info. I trust it ( because she does ) but I can't really say it's more than just my faith in her to do her homework and find legit sources..
Here it is:
New Concerning Variant: B.1.1.529
I hope everyone in the States had a fantastic Thanksgiving (even if you're a Dallas Cowboys football fan). I hate to ruin the holiday, but…
We have a new variant. I've not seen this much anxiety ridden chatter among scientists about a COVID19 variant before. Even among the calm, cool, and collected scientists.
(This post is copy and pasted from my newsletter, which is way easier to read than FB. It also has all of the figures and hyperlinks embedded.
View the newsletter here:
https://yourlocalepidemiologis......)
***What happened this week?***
This week we (epidemiologists and virologists) have been closely following a new COVID19 mutation. Three days ago it was designated the name B.1.1.529.
As I write this, the WHO TAG team is convening. They are tasked to do three things:
1. Review the evidence to determine if B.1.1.529 is, in fact, a threat;
2. Classify whether the new variant is a "variant of interest" (in other words, hypothesize that this variant is a threat, but we don't have the evidence yet) or a "variant of concern" (we have scientific evidence that this variant is a threat);
3. Name the variant. The next Greek name in line is "Nu".
The name and classification will hit the news cycle once WHO officially announces. Whatever its name, this is what we know thus far…
***What is the B.1.1.529 variant?***
B.1.1.529 was first discovered in Botswana on November 11. It was then quickly identified in South Africa three days later and identified in two cases in Hong Kong. This morning Israel and Belgium announced that they have cases. The Belgium case was a young, unvaccinated woman who developed flu-like symptoms 11 days after travelling to Egypt via Turkey. She had no links to South Africa. This means that the virus is already circulating in communities. As of yesterday, 100 cases have been identified across the globe (mostly in South Africa). As I write this, no cases have been identified in the United States.
B.1.1.529 has 32 mutations on the spike protein alone. This is an insane amount of change. As a comparison, Delta had 9 changes on the spike protein. We know that B.1.1.529 is not a "Delta plus" variant. The figure below shows a really long line, with no previous Delta ancestors. So this likely means it mutated over time in one, likely immunocompromised, individual (see my P.S. note at the end of the post).
Nonetheless, we always pay attention to changes on the spike protein because the spike is the key into our cells. If the virus changes to become a smarter key, we need to know. We are particularly interested in mutations that could do any of the following:
-Increase transmissibility;
-Escape our vaccines or infection-induced immunity; and/or
-Increase severity (hospitalization or death).
B.1.1.529 has the potential to do all three. We know this because we've seen a number of these mutations on other variants of concern (VOC), like Delta, Alpha, and Gamma. Dr. Jeffrey Barrett listed the mutations in a figure below. Each row represents a different mutation (32 total). The left hand column is the location of the change. The right hand column/color correspond to what we know (or don't know) about the change.
-Red: This means bad. There are nine mutations on B.1.1.529 that we've seen in previous Variants of Concern (VOC). P681R is particularly bad news.
-Purple: These are new mutations (i.e. not seen in other VOC), but we have lab data to suggest they are a threat.
-Yellow: These probably mean something because of their location, but we don't know what they mean yet. They have not been previously seen in VOC
-Blue: We've never seen these changes before. They may mean something or may mean nothing. We don't know yet. We need more data.
-Green: This is a mutation that's been present on all of the variants since early 2020. Not to be of concern.
Of these, some mutations have properties to escape antibody protection (i.e. outsmart our vaccines and vaccine-induced immunity). There are several mutations association with increased transmissibility. There is a mutation associated with increased infectivity. This slide, from a presentation yesterday from the South Africa Health Ministry, summarized B.1.1.529 nicely.
It will take weeks to understand what these new mutations mean or, more importantly, the combination of so many mutations. Keep in mind that the number of mutations does NOT always equal more severe. While these important lab studies are under way, we can watch carefully what's happening in the "real world".
***What we're seeing in the real world?***
*Individual-level data*
We know a lot about the Hong Kong cases because of their impeccable contact tracing. Health authorities published a report of these two cases yesterday.
The first case in Hong Kong was a 36 year old, fully vaccinated (two Pfizer doses in May/June 2021) male. He was traveling through South Africa from October 22 to November 11. Before returning to Hong Kong, he tested negative on a PCR. As per usual, once he landed in Hong Kong he was required to quarantine. On day 4 of quarantine (November 13), he tested positive on a PCR.
Another guest across the hallway was also infected with B.1.1.529. He was Pfizer vaccinated in May/June 2021 too. In both of these rooms, 25 out of 87 swabs were positive for the virus.
These Hong Kong cases tell us two things:
-Confirms that COVID19 is airborne (we knew this)
-During their PCR tests, the viral loads were VERY high considering they were negative on previous PCR tests. They had a Ct value of 18 and 19 value. So, this tell us that B.1.1.529 is likely highly contagious.
*Population-Level Data*
There are preliminary signs that B.1.1.529 is driving a new wave in South Africa. Health officials are looking particularly at a region called Gauteng. In just one week, test positivity rate increased from 1% to 30%. This is incredibly fast.
If we zoom out on South Africa as a whole, we see cases starting to exponentially increase. On Tuesday there were 868 cases, Wednesday there were 1,275 cases, Thursday there were over 3,500 cases. We do not know if these cases are all B.1.1.529, but the timing of explosive spread is suspect.
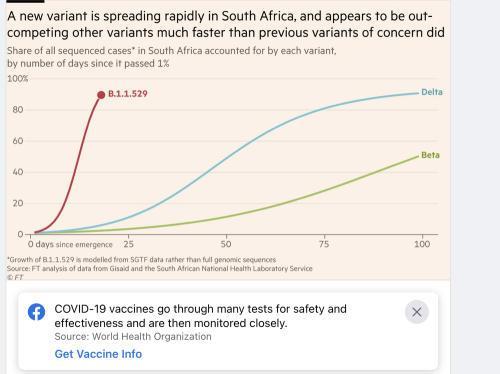
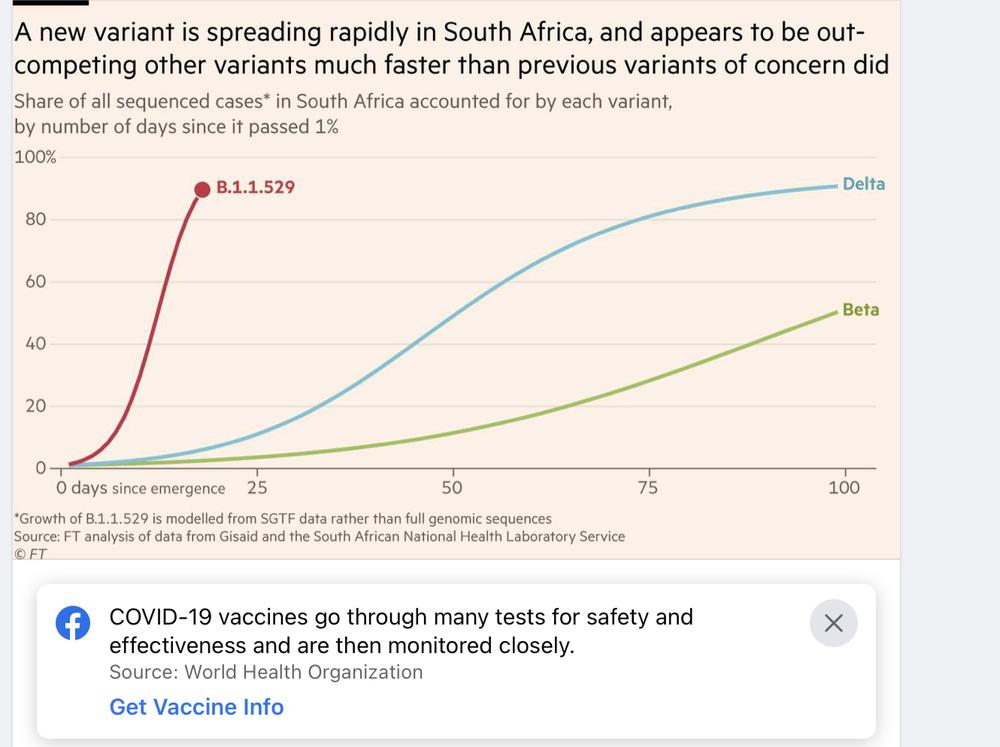
The rate in which these cases are spreading are far higher than any previous variant. Disease modeling scientist Weiland estimated that B.1.1.529 is 500% more transmissible than the original Wuhan virus. (Delta was 70% more transmissible). John Burn-Murdoch (Chief Data Reporter at Financial Times) also found that B.1.1.529 is much more transmissible than Delta. He plotted the spread below.
***There is some good news though***
First, we can detect B.1.1.529 on a PCR test. This typically isn't the case. Usually a swab would have to go to a special lab for genome sequencing to know which variant caused the infection. However, it looks like B.1.1.529 has a special signal like Alpha on the PCR directly. For example, when the PCR is positive it lights up two channels instead of three channels, indicating that it's B.1.1.529. This is amazing news because it means we can track this virus much easier and much quicker around the world.
Second, we caught this virus incredibly early. I can't stress enough how amazing South Africa has been on communicating and taking hold of the situation. Because of their swift response, scientists around the world are already working together to decode this new threat. Early detection means that we have a surveillance system in place and it's working.
Third, if we need another vaccine, we can do this incredibly quickly. Thanks to the new biotechnology, mRNA vaccines are really easy to alter. Once the minor change is made, only 2 dozen people need to enroll in a trial to make sure the updated vaccine works. Then it can be distributed to arms. Because the change is small, an updated vaccine doesn't need Phase III trials and/or regularity approval. So, this whole process should take a max of 6 weeks. We haven't heard from Moderna or Pfizer if they've started creating an updated vaccine, but I guarantee conversations have started behind closed doors.
***Bottom Line***
There's still so much that we don't know but what we do know is incredibly concerning. We are in a lull right now as we wait for scientific evidence to answer two questions as soon as possible:
1. Does B.1.1.529 escape vaccines like we fear?
2. Does B.1.1.529 continue to outcompete Delta like we're seeing in South Africa?
Once we have answers to these two questions, we'll know the next step. Stay tuned.
Love, YLE
P.S. A few random thoughts I didn't know where to put above:
1. Travel bans are not evidence-based: It may seem like travel bans for individual countries are a necessary step, but I cannot stress enough that they do not work. For example, we had a travel ban with China in March 2020, only to be infiltrated with a European strain. Travel bans are a political move; a tool to show the public that the government is responding. Travel bans can do a lot of damage, though, like perpetuate disease related stigma. This variant has already spread. A travel ban is not an evidence-based solution.
2. Individual-level protection. None of this variant stuff changes what you need to do on an individual-level right now. Unless, of course, if you weren't doing anything at all. Get vaccinated. Get boosted. Ventilate spaces. Use masks. Test if you have symptoms. Isolate if positive. And encourage others to do the same.
3. Immunocompromised: It looks like this variant has major implications of virus evolution in immunocompromised hosts. This underscores the need to ensure that immunocompromised people are protected by their communities. Not just for their sake, but for all of ours.
May be an image of text that says 'A new variant is spreading rapidly in South Africa, and appears to be out- competing other variants much faster than previous variants of concern did Share of all sequenced cases* in South Africa accounted for by each variant, by number of days since it passed 1% 100% 80 B.1.1.529 60 40 Delta 20 Beta 0 days since emergence 25 Growth B.1. 529 is modelled from SGTF data rather than full genomic sequences Source: FT analysis of data from Gisaid and the South African National Health Laboratory Service ©FT 50 75 100'
COVID-19 vaccines go through many tests for safety and effectiveness and are then monitored closely.
Source: World Health Organization
Here's the graph that was attached ..it would not load properly